






Adalia HealthCare offers a high standard medical service on Cardiology, Cardiovascular Diseases and Coronary Heart Diseases performed
by
Prof Cengiz Ermis, MD
Cardiologist, Cardiac Electrophysiologist
from Antalya Akdeniz University Faculty of Medicine

Prof Ermis finished his medical training at Akdeniz University Faculty of Medicine. He, then completed his cardiology fellowship at the same instution. In year 2001 he started his Cardiac Electrophysiology fellowship at the University of Minnesota Medical School in USA. Upon completion of this subspecialty training he returned back to Akdeniz University, Faculty of Medicine. He became associate professor in 2005 and received promotion to full professor position in 2010. He is currently a member of Department of Cardiology. Apart from his experience in invasive Cardiology, Cardiovascular Diseases and Coronary Heart Diseases , his professional medical specialization is Cardiac Arrhythmia. He is one of the handful distingushed Cardiac Electrophysiologists in Turkey .
All interventions and operations are performed in the best equipped , JCI approved hospitals in Antalya which closely and exclusively associate with Adalia HealtCare.
A brief information about Cardiovascular diseases
Cardiovascular disease is a class of diseases that involve the heart or blood vessels (arteries, capilaries and veins ).

Cardiovascular disease refers to any disease that affects the cardiovascular system, principally cardiac disease, vascular diseases of the brain and kidney, and peripheral arterial disease. The causes of cardiovascular disease are diverse but atherosclerosis and/or hypertension are the most common. Besides, with aging come a number of physiological and morphological changes that alters cardiovascular function and lead to subsequently increased risk of cardiovascular disease, even in healthy asymptomatic individuals.
Cardiovascular diseases remain the biggest cause of deaths worldwide, though over the last two decades, cardiovascular mortality rates have declined in many high-income countries. At the same time cardiovascular deaths and disease have increased at a fast rate in low- and middle-income countries. Although cardiovascular disease usually affects older adults, the antecedants of cardiovascular disease, notably atherosclerosis begin in early life, making primary prevention efforts necessary from childhood. There is therefore increased emphasis on preventing atherosclerosis by modifying risk factors, such as healthy eating,exercise, and avoidance of smoking.
Types
- Coronary heart disease (also ischaemizc heart diesease or coronary artery disease)
- Cardiomyopathy – diseases of cardiac muscle
- Hypertensive heart disease – diseases of the heart secondary to high blood pressure
- Heart failure
- Corpulmonale – a failure of the right side of the heart
- Cardiac dysrhythmias – abnormalities of heart rhythm
- Inflammatory heart disease
- Endocarditis-inflammation of the inner layer of the heart, the endocardium. The structures most commonly involved are the heart valves.
- Inflammatory cardiomegaly
- Myocarditis-inflammation of the myocardium, the muscular part of the heart
- Valvular heart disease
- Stroke and cerebrovascular disease
- Peripheral arterial disease
Risk factors
Almost all cardiovascular disease in a population can be explained in terms of a limited number of risk factors: age, gender, high blood pressure, high serum cholesterol levels, tobacco smoking, excessive alcohol consumption, family history, obesity, lack of physical activity, psychosocial factors, diabetes mellitus, air pollution. While the individual contribution of each risk factor varies between different communities or ethnic groups the consistency of the overall contribution of these risk factors is remarkably strong. Some of these risk factors, such as age, gender or family history are immutable, however many important cardiovascular risk factors are modifiable by lifestyle change, drug treatment or social change.
Age
Age is an important risk factor in developing cardiovascular diseases. It is estimated that 87 percent of people who die of coronary heart disease are 60 and older. At the same time, the risk of stroke doubles every decade after age 55.
Multiple explanations have been proposed to explain why age increases the risk of cardiovascular diseases. One of them is related to serum cholesterol level. In most populations, the serum total cholesterol level increases as age increases. In men, this increase levels off around age 45 to 50 years. In women, the increase continues sharply until age 60 to 65 years.
Aging is also associated with changes in the mechanical and structural properties of the vascular wall, which leads to the loss of arterial elasticity and reduced arterial compliance and may subsequently lead to coronary artery disease.
Sex
Men are at greater risk of heart disease than pre-menopausal women. However, once past menopause, a woman’s risk is similar to a man’s.
Among middle-aged people, coronary heart disease is 2 to 5 times more common in men than in women. In a study done by the World Health Organization, sex contributes to approximately 40% of the variation in the sex ratios of coronary heart disease mortality.
Pathophysiology
Population based studies show that atherosclerosis the major precursor of cardiovascular disease begins in childhood. The Pathobiological Determinants of Atherosclerosis in Youth Study demonstrated that intimal lesions appear in all the aortas and more than half of the right coronary arteries of youths aged 7–9 years.
This is extremely important considering that 1 in 3 people will die from complications attributable to atherosclerosis. In order to stem the tide education and awareness that cardiovascular disease poses the greatest threat and measures to prevent or reverse this disease must be taken.
Prevention
Measures to prevent cardiovascular disease may include:
- a low-fat, high-fiber including whole grains and plenty of fresh fruit and vegetables (at least five portions a day)
- a diet high in vegetables and fruit
- tobacco cessation and avoidance of second-hand smoke;
- limit alcohol consumption to the recommended daily limits; consumption of 1-2 standard alcoholic drinks per day may reduce risk by 30% However excessive alcohol intake increases the risk of cardiovascular disease.
- lower blood pressures, if elevated, through the use of antihypertensive medications;
- decrease body fat (BMI) if overweight or obese;
- increase daily activity to 30 minutes of vigorous exercise per day at least five times per week;
- decrease psychosocial stress.
Cardiac Arrhythmia
What Is Cardiac Arrhythmia?
A cardiac arrhythmia is any irregularity in the heart beat. This includes:
- Abnormally fast heartbeats (Tachycardia)
- Abnormally slow heartbeats (Bradycardia)
- Extra beats
- Skipped beats (Premature contraction)
Most people with an arrhythmia have nothing to worry about. For others, an arrhythmia may be a dangerous condition that requires medical treatment.
 The most common type of arrhythmia is atrial fibrillation, a potential serious condition. It occurs when the heart’s two small upper chambers (the atria) quiver instead of beating, allowing blood to pool inside and clot.
The most common type of arrhythmia is atrial fibrillation, a potential serious condition. It occurs when the heart’s two small upper chambers (the atria) quiver instead of beating, allowing blood to pool inside and clot.
Causes
Some people are born with conditions that cause arrhythmias and others develop them with age or when scar tissue occurs after a heart attack or years of hypertension. As the population ages, they are becoming more common. Some arrhythmias may also be made worse by diet (especially caffeine), exertion or emotional issues.
Diagnosis
- Irregular heart beat or heart fluttering
- Heart palpitations or rapid thumping inside the chest
- Dizziness, sweating and chest pain or pressure
- Shortness of breath
- Excessive tiredness when exercising
Doctor may be able to detect an arrhythmia by listening to the heart with a stethoscope. The following tests may also be ordered:
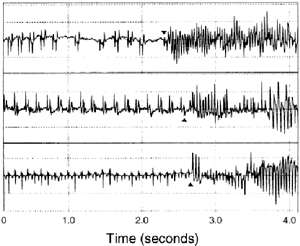
- Electrocardiogram (EKG or ECG) – This test, which involves attaching (with adhesive material) small electrodes to the arm, leg and chest to measure the rate and regularity of a heartbeat, may be taken while the patient is resting or after exercising on a treadmill.
- Holter-monitoring – This test is essentially a portable electrocardiogram, which records changes in heart rhythm as a person goes about daily activities.
- Transtelephonic monitoring – The patient wears EKG electrodes for several days or several weeks, but instead of recording the heartbeat activity directly, the patient calls a monitoring station whenever he or she feels an arrhythmia.
- Cardiac catheterization– A thin flexible tube (catheter) is passed through an artery in the groin or arm into the coronary arteries to monitor blood pressure and blood flow.
Treatment
Many arrhythmias require no treatment at all. Serious arrhythmias may be treated with one or more of the following options:
- Medications – to help regulate the heartbeat or to prevent complications such as stroke
- Cardioversion – an electric shock administered through a defibrillator to slow down or regulate a heartbeat (patient is anesthetized)
- Cardiac catheter ablation (Elektrophysiology) – an electrophysiologist uses a special catheter to pinpoint and eliminate the abnormal electrical pathways in a patient’s heart.
- Automatic implantable defibrillator – a device surgically implanted inside the patient’s chest, which monitors the heart’s rhythm and provides an electric shock, if necessary, to slow down or regulate the heartbeat
- Artificial pacemaker – an electrical device placed under the skin that sends electrical signals to the heart to make the heart beat
- Surgery– to remove or repair heart tissue
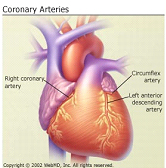
What Is Coronary Heart Disease?
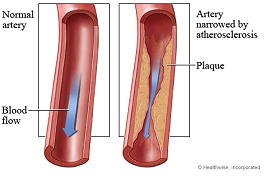
Coronary heart disease (CHD) is a disease in which a waxy substance called plaque (plak) builds up inside the coronary arteries. These arteries supply oxygen-rich blood to your heart muscle.
When plaque builds up in the arteries, the condition is called atherosclerosis. The buildup of plaque occurs over many years.
Causes
Coronary heart disease (CHD) is the leading cause of death in the world in modern times for men and women.
Coronary heart disease may also be called hardening of the arteries.
- Fatty material and other substances form a plaque build-up on the walls of your coronary arteries. The coronary arteries bring blood and oxygen to your heart.
- This buildup causes the arteries to get narrow.
- As a result, blood flow to the heart can slow down or stop.
Symptoms
Symptoms may be very noticeable, but sometimes you can have the disease and not have any symptoms. This is especially true in the early stages of heart disease.
Chest pain or discomfort (angina) is the most common symptom. You feel this pain when the heart is not getting enough blood or oxygen. How bad the pain is varies from person to person.
- It may feel heavy or like someone is squeezing your heart. You may feel it under your breast bone (sternum), but also in your neck, arms, stomach, or upper back.
- The pain usually occurs with activity or emotion, and goes away with rest or a medicine called nitroglycerin.
- Other symptoms include shortness of breath and fatigue with activity (exertion).
Women, elderly people, and people with diabetes are more likely to have symptoms other than chest pain, such as:
- Fatigue
- Shortness of breath
- General weakness
Exams and Tests
Tests may include:
- Coronary angiography — an invasive test that evaluates the heart arteries under x-ray
- Echocardiogram stress test
- Electrocardiogram (ECG)
- Electron-beam computed tomography (EBCT) to look for calcium in the lining of the arteries — the more calcium, the higher your chance for CHD
- Exercise stress test
- Heart CT scan
- Nuclear stress test
Treatment
Treatment depends on your symptoms and how severe the disease is.
Procedures and surgeries used to treat CHD include:
- Angioplasty and stent placement, called percutaneous coronary interventions (PCIs)
- Coronary artery bypass surgery
- Minimally invasive heart surgery
An additional information about Coronary Angiography
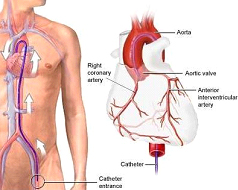
Coronary angiography is a procedure that uses a special dye (contrast material) and x-rays to see how blood flows through the arteries in patient’s heart.
How the Test is Performed
Coronary angiography is usually done along with cardiac catheterization.Before the test starts, Patient will be given a mild sedative to help you relax. An area of his body, usually the arm or groin, is cleaned and numbed with a local numbing medicine (anesthetic). The cardiologist passes a thin hollow tube, called a catheter, through an artery and carefully moves it up into the heart. X-ray images help the doctor position the catheter.
Once the catheter is in place, dye (contrast material) is injected into the catheter. X-ray images are taken to see how the dye moves through the artery. The dye helps highlight any blockages in blood flow.
The procedure may last 30 to 60 minutes.
Why the Test is Performed
Coronary angiography may be done if patient experiences:
- Angina for the first time
- Angina that is becoming worse, not going away as fast, occurring more often, or happening at rest (called unstable angina,)
- Aortic stenosis
- Atypical chest pain, when other tests are normal
- Had an abnormal heart stress test
- To have surgery on your heart and you are at high risk for coronary artery disease
- Heart failure
- Recent heart attack
Normal Results :There is a normal supply of blood to the heart and no blockages.
What Abnormal Results Mean : An abnormal result may mean you have a blocked artery. The test can show how many coronary arteries are blocked, where they are blocked, and the severity of the blockages.
An additional information about Coronary Angioplasty
Coronary angioplasty is a procedure carried out to help relieve the stress on arteries, sometimes the arteries and blood vessels leading to and from the heart get clogged or blocked. This happens mainly in those over 30, but it is not unheard of in younger people. When the arteries get clogged or partially blocked, it is called atherosclerosis.
Who needs a Coronary Angioplasty
Often, people go to the doctor complaining of angina (chest pain), or being short of breath.
These can be symptoms of atherosclerosis. The doctor will order tests to find out if the heart is getting the proper flow in and out.
There are a number of tests which can be done to see if the arteries are blocked or completed occluded.
One common test is a dye contrast and is done routinely for many conditions.
An I.V. will be started and a dye will be injected just before the patient goes into a CT scan.
If the patient is found to have blocked arteries, there are several methods of treatment, one of those methods is Coronary Angioplasty.
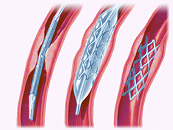
What is done in a Coronary Angioplasty
In short; doctor can use a stent or a balloon like device to open up the artery. Patient is normally awake during the procedure and given a general anesthetic. Using a long, flexible tube, the medical surgical team goes in to the femoral (leg) artery and pushes the tube up until it reaches the affected artery. Dye contrasting x-rays are done to let doctor know the size of the artery and other information. Then a small wire is inserted through the catheter that is in the leg. The balloon is inflated and the stent left in place, thereby opening up the artery for blood to flow freely.

